
Dr Rory Dewhurst Case Study: Achieving Good Aesthetic Outcomes With Fixed Aesthetic Orthodontics
Dr Rory Dewhurst addresses an anterior open bite with occlusal cant with the use of aesthetic micro-coated orthodontic archwire and polycrystalline ceramic brackets.
This orthodontic restorative case demonstrates the use of aesthetic micro-coated orthodontic archwire and polycrystalline ceramic brackets to address an anterior open bite with occlusal cant. The case was finished with subsequent whitening and restoration of a microdont maxillary lateral incisor.
Introduction
The use of ceramic brackets and coated archwires is an aesthetic orthodontic treatment option for the increasing number of patients seeking orthodontic treatment. Aesthetic coated archwires have been shown to aid sliding mechanics of orthodontic systems by reducing bracket friction when compared to uncoated wires (Farronato et al, 2012), which has implications of reducing anchorage demands and treatment times. Low orthodontic forces are preferable to move teeth, in order to avoid increased treatment time and other unwanted side effects.
Some studies suggest polytetrafluoroethylene (PTFE) coated archwires have been shown to exert reduced force on deflection when compared to uncoated wires, although others demonstrate little statistical difference between the two materials (Bącela et al, 2020).
Case study
A 24-year-old patient presented with a class II division I malocclusion on a class I skeletal base. This was complicated by:
• Mild crowding in the maxillary and mandibular arches
• Anterior open bite with canted maxillary plane
• Half unit class II molar relationship left side with unilateral buccal crossbite
• Dark but vital microdont upper right lateral incisor.
The patient was primarily concerned about the aesthetic appearance of their teeth and wished to avoid extraction based orthodontics. As a result, they opted for labial fixed appliance therapy using ceramic brackets with PTFE microcoated Euroline archwire. In addition to the orthodontic component of their treatment, the patient also proceeded to undergo tooth whitening and composite restoration of the upper right lateral incisor. The main orthodontic treatment aims were to ensure optimal alignment and levelling of gingival margins, in addition to correction of the occlusal cant. I planned to establish a positive overbite and reduce the patient’s overjet, accepting the current molar relationships.
Due to risk of relapse, lifelong retention at treatment completion was recommended. The specific concerns of potential limited reduction of anterior open bite, subsequent risk of relapse and potential loss of vitality of the upper right lateral incisor were discussed with the patient. Referral for orthognathic surgery, fixed lingual and fixed labial appliance therapy and removable aligner treatment options were also offered and considered.
Wire sequence
• 0.012 nickel titanium upper and lower, with removal of existing composite restoration from upper right lateral incisor
• 0.018 nickel titanium upper, 0.014 nickel titanium lower
• 0.018 x 0.025 nickel titanium upper, 0.018 nickel titanium lower
• Upper 0.018 x 0.025 stainless steel, 0.020 stainless steel lower with 4.5oz, 1/4’ anterior elastics, followed by 2.5oz, 1/8’ anterior and box elastic during finishing • Bonded retention (Ortho Flextech stainless steel chain) and thermoformed retainers for nightly wear following post-orthodontic tooth whitening, and composite (Enamel Plus HFO) restoration of the upper right lateral incisor.
 Full face, preoperative.
Full face, preoperative.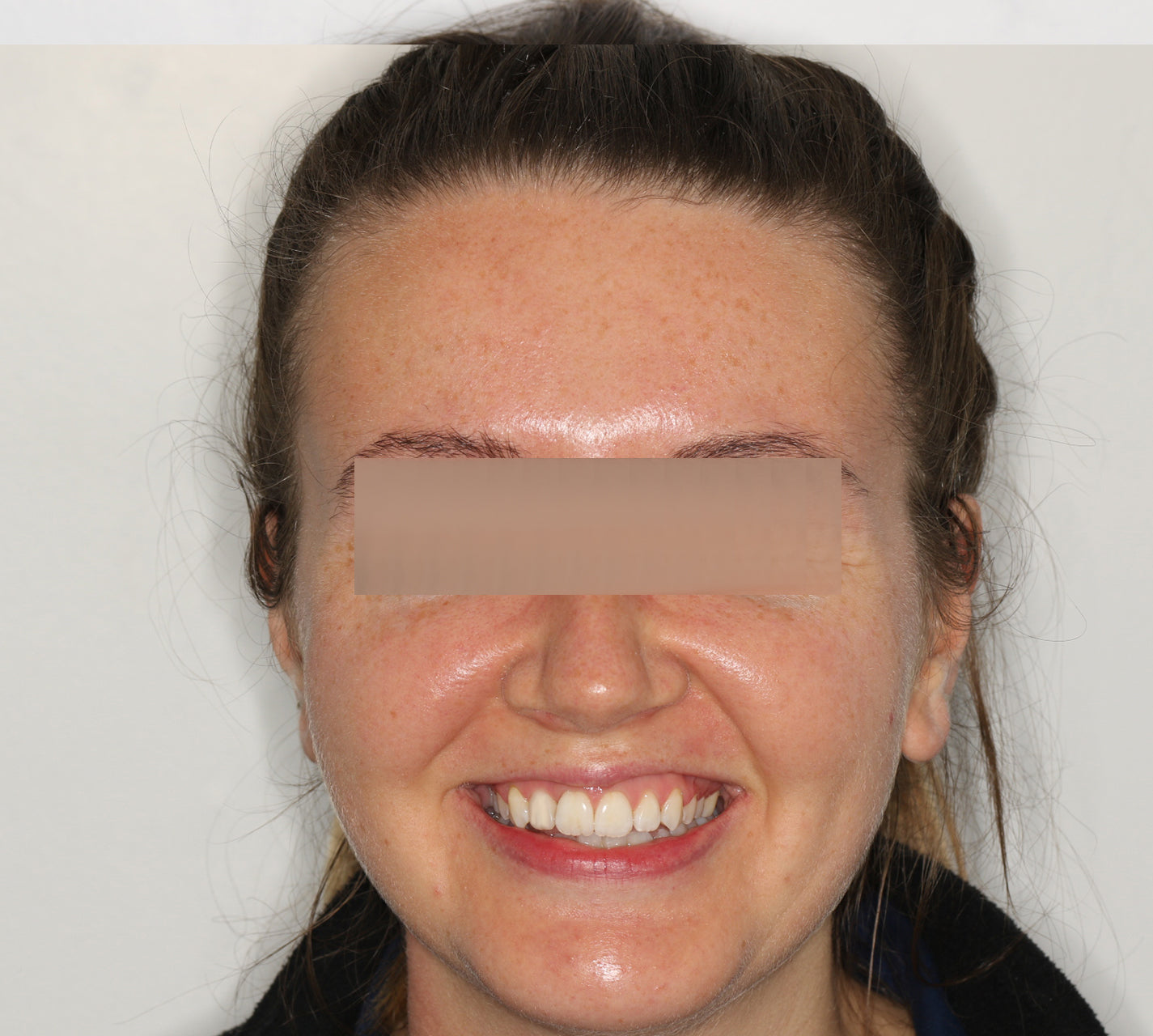 Full face, postoperative.
Full face, postoperative. Anterior view, during treatment.
Anterior view, during treatment. Anterior view, during treatment.
Anterior view, during treatment. Anterior retracted, preoperative.
Anterior retracted, preoperative. Anterior view, postoperative.
Anterior view, postoperative. Upper occlusal, preoperative
Upper occlusal, preoperative Upper occlusal, postoperative.
Upper occlusal, postoperative. Lower occlusal, preoperative.
Lower occlusal, preoperative. Lower occlusal, postoperative.
Lower occlusal, postoperative.
Treatment reflection
As seen in the clinical photographs, the use of aesthetic ceramic brackets and micro-coated wires provided sufficient slide mechanics to facilitate alignment and levelling of teeth and the aesthetic result the patient wanted to achieve. The use of these materials also avoided the unaesthetic appearance of metal brackets and wires.
However, I reflect that the process of wire bending and incorrect brushing technique resulted in episodic chipping of the wire micro-coating, which could have been minimised with improved initial bracket positions and additional patient education.
Having achieved the treatment aim of a positive overbite, further overbite correction could have been achieved with the introduction of posterior bite blocks. This would have increased the degree of molar intrusion relative to incisor extrusion and reduced the risk of anterior open bite relapse.
Orthodontic leveling has corrected the occlusal cant as planned, and achieved symmetrical gingival zenith positions for the upper anterior teeth. The unintended consequence of this was that the position of the mesial gingival papillae of the upper right lateral incisor is more apical compared to the left.
This asymmetry impacts on the final aesthetics of the case. If I were to approach a similar scenario again, I would re-evaluate the degree of intrusion at the levelling stage and instead consider a combined approach of orthodontic levelling with either gingivectomy or surgical crown lengthening to achieve symmetry of both the zenith positions and the height of papillae.
From an extraoral perspective, one could also consider the use of botulinum toxin to reduce the increased degree of lip activity on the left side compared to the right side. This would be in keeping with the patient’s priorities for a more symmetrical smile. Overall, the patient was pleased with the treatment modality selected and the final aesthetic result. Treatment time was extended from the planned 10 months to approximately 15 months as a result of changes to working schedules related to the SARS-CoV-2 pandemic.
Conclusion
Ceramic brackets and micro-coated wires are an aesthetic fixed appliance option that can be used to achieve good aesthetic outcomes. Accurate preoperative and continuous mid-treatment assessment of gingival and tooth position is essential to achieving the best aesthetic outcome for patients. Patient satisfaction can be considered the most important factor when evaluating treatment end points.


About Rory Dewhurst
DR RORY DEWHURST BDS (HONS) FRACDS (GDP) PGCERT (ORTHGP) Rory qualified from the Cardiff University School of Dentistry in 2011, where he was a recipient of the Jayne Hodge Foundation Prize. He has since worked in both general practice and the oral and maxillofacial surgery department at Morriston Hospital, Swansea. He is currently based in Bristol and Cardiff in private cosmetic practice. Rory has completed the Postgraduate Certificate in Orthodontics in General Practice.
About DB Orthodontics
It is our company mission to become a global leader in orthodontic and laboratory supplies. With over 45 years of experience in orthodontics, we recognise the importance of quality, service and innovation. Working to ISO13485 standards we strive for perfection in all that we do, from unique product design to the excellent service provided by our dedicated customer service and sales teams. We are continually developing our product range, designing innovative products through consultation with leading orthodontists from the world, to ensure that our products meet the high standards expected by today’s practitioners.
